Day 10
We couldn't believe it was already Saturday. Our last day in the operating room had crept up on us so quickly. We had only one surgery scheduled for today, however if had the potential to be a substantial case. 16 year-old Sheila has spastic cerebral palsy, a neurological disorder caused by injury to the brain in the perinatal period leaving her non-communicative and non-ambulatory. As a result, her body is tightly curled into the fetal position due to the imbalance between her flexor and extensor muscles. Because of this muscle imbalance, her spine has developed a severe deformity making it near impossible for her mother to provide care and personal hygiene, and rendering her unable to sit up even with a brace or some form of support. Sheila's mother carries her daughter draped over her arms. The girl is grotesquely undernourished, a clear sign that feeding her is difficult. Finally, Sheila is in constant pain as manifest by her heartbreaking wail.
We couldn't believe it was already Saturday. Our last day in the operating room had crept up on us so quickly. We had only one surgery scheduled for today, however if had the potential to be a substantial case. 16 year-old Sheila has spastic cerebral palsy, a neurological disorder caused by injury to the brain in the perinatal period leaving her non-communicative and non-ambulatory. As a result, her body is tightly curled into the fetal position due to the imbalance between her flexor and extensor muscles. Because of this muscle imbalance, her spine has developed a severe deformity making it near impossible for her mother to provide care and personal hygiene, and rendering her unable to sit up even with a brace or some form of support. Sheila's mother carries her daughter draped over her arms. The girl is grotesquely undernourished, a clear sign that feeding her is difficult. Finally, Sheila is in constant pain as manifest by her heartbreaking wail.
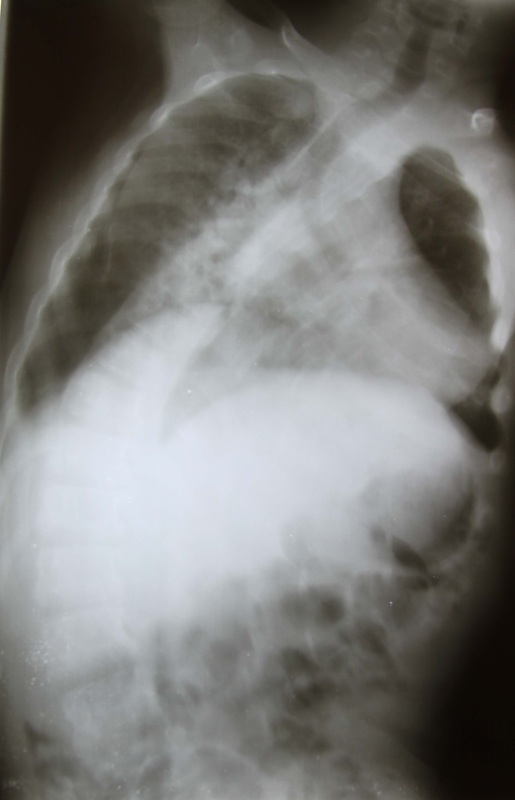
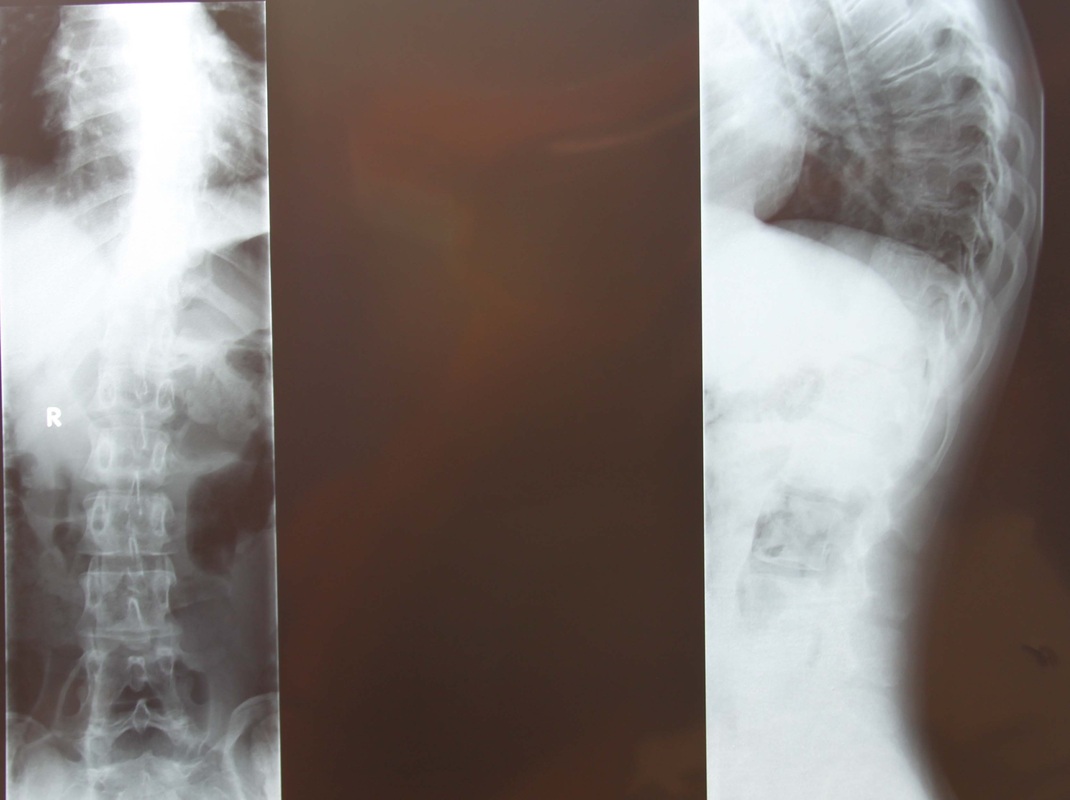
Sheila's x-rays
While Sheila will never regain the use of her muscles, nor will she ever walk, Dr. Lieberman could still use metal screws and wires to reduce the curve in her spine and to allow her to sit upright. This would tremendously reduce her mother's burden as caregiver. It might also even help with some of Sheila's pain.
Our morning got off to a good start; we were even ahead of schedule... until Zvi jinxed us by commenting on just that. Within five minutes the entire hospital lost power, delaying our start time. Power returned to the operating rooms within half an hour but the rest of the hospital was still in the dark. The head nurse of the surgical ward even borrowed an outlet in our operating room to boil eggs for her lunch.
Our morning got off to a good start; we were even ahead of schedule... until Zvi jinxed us by commenting on just that. Within five minutes the entire hospital lost power, delaying our start time. Power returned to the operating rooms within half an hour but the rest of the hospital was still in the dark. The head nurse of the surgical ward even borrowed an outlet in our operating room to boil eggs for her lunch.

Our operating theatre in Mbarara doubled as a kitchen while power was lost throughout the hospital
Sheila's operation took almost 5 hours. As Dr. Lieberman revealed the spinous processes of Sheila's spine (the parts the form the bumps under your skin), he made an unfortunate discovery. Because she is unable to bear weight and likely deficient in vitamin D, Sheila's bone was very soft. Worse yet, it wasn't clear that her soft bone could withstand the pressure of the metal wires even after she had healed. Past the point of no return, Dr. Lieberman finished the surgery and Sheila was sent to the ICU.
Sheila's case exemplified some of the ethical dilemmas in surgery, and so our lesson of the day revolved around her. Unlike our other cases from this week, Sheila's operation was not expected to provide significant symptomatic relief. When I asked Dr. Lieberman what the goal of surgery was, he explained that sometimes you have to adopt a perspective that includes the suffering of the patient's family. In Sheila's case, her mother was unable to properly care for her in her current state. Perhaps a straighter spine would allow Sheila to prop herself up and eat, thus improving both her and her mother's quality of life.
Having just completed our last surgery, the team packed up the operating room and stored our equipment for pick-up the next day. After rounding on some of our patients, we left the hospital for our final dinner in Mbarara. We were joined by Dr. Joseph, a surgical trainee at the hospital, and by our trusted middle man, Metu, who takes care of all the shipping and receiving for the mission. Back at the hotel later that evening, the team sat with a bottle of wine and some beers and reflected on a very productive and rewarding week. We shuffled off to bed, each one wishing this had not been our last operating day.
Sheila's case exemplified some of the ethical dilemmas in surgery, and so our lesson of the day revolved around her. Unlike our other cases from this week, Sheila's operation was not expected to provide significant symptomatic relief. When I asked Dr. Lieberman what the goal of surgery was, he explained that sometimes you have to adopt a perspective that includes the suffering of the patient's family. In Sheila's case, her mother was unable to properly care for her in her current state. Perhaps a straighter spine would allow Sheila to prop herself up and eat, thus improving both her and her mother's quality of life.
Having just completed our last surgery, the team packed up the operating room and stored our equipment for pick-up the next day. After rounding on some of our patients, we left the hospital for our final dinner in Mbarara. We were joined by Dr. Joseph, a surgical trainee at the hospital, and by our trusted middle man, Metu, who takes care of all the shipping and receiving for the mission. Back at the hotel later that evening, the team sat with a bottle of wine and some beers and reflected on a very productive and rewarding week. We shuffled off to bed, each one wishing this had not been our last operating day.
Day 11
Move out day. After a leisurely breakfast at the hotel, Izzy, Zvi, Rob and Dani left for the hospital for a final review of the patients. There they met with Dr. Deo and Dr. Joeseph and as a team changed all the dressings, pulled all the catheters, and provided last minute therapy and discharge instructions. At the hospital, Rob immediately began retrieving our equipment from storage and loading it with Mr. Metu and his team onto the delivery truck. When all packed, the four made their way back to the hotel to meet up with Sherri and Jen. The six of us then loaded our luggage onto the truck and started the nearly eight hour drive back to Entebbe.
Along the way, we stopped at Lake Mboro National Game Reserve. We spent over two hours driving though the park, taking photos of zebras, warthogs, monkeys, and other indigenous wildlife. It was our first and only tourist experience inside Uganda!
Move out day. After a leisurely breakfast at the hotel, Izzy, Zvi, Rob and Dani left for the hospital for a final review of the patients. There they met with Dr. Deo and Dr. Joeseph and as a team changed all the dressings, pulled all the catheters, and provided last minute therapy and discharge instructions. At the hospital, Rob immediately began retrieving our equipment from storage and loading it with Mr. Metu and his team onto the delivery truck. When all packed, the four made their way back to the hotel to meet up with Sherri and Jen. The six of us then loaded our luggage onto the truck and started the nearly eight hour drive back to Entebbe.
Along the way, we stopped at Lake Mboro National Game Reserve. We spent over two hours driving though the park, taking photos of zebras, warthogs, monkeys, and other indigenous wildlife. It was our first and only tourist experience inside Uganda!

Zebras at the Lake Mboro National Park

Lake Mboro
We made it to Entebbe eight hours later with numb bottoms and empty stomachs. In our usual fashion, we discussed the lessons of the day over dinner at the hotel.
With the long drive back to Entebbe to reflect on my experience on the Mission, I realized I had witnessed some of the best leadership and team building skills I have seen yet. Dr. Lieberman is as natural a leader as they come, and from watching him and his surgical team over the past week, I recognized the skills that make an effective team leader: expertise that commands respect; teaching methods that drive pupils to want to know more; organizational skills and the ability to coordinate a network of moving parts; setting an example of patience and perseverance in the face of challenges and setbacks; encouraging team members to reflect on their own learning and their roles within the team; and finally, the acuity to select members of team that have their own expert skill sets and personality types that mesh together naturally. That was one of the most valuable and translatable lessons I learned during my two weeks with the Uganda Spine Surgery Mission.
So that's it! Time to sign off. Tomorrow the team flies back to London and then on to our respective home cities. It was a privilege to be part of the 2013 Spine Surgery Mission, and I look forward to hearing about all the successes of the 2014 trip!
Quotes of the day:
"We still have a wottle of bine"
"Six numb bums"
With the long drive back to Entebbe to reflect on my experience on the Mission, I realized I had witnessed some of the best leadership and team building skills I have seen yet. Dr. Lieberman is as natural a leader as they come, and from watching him and his surgical team over the past week, I recognized the skills that make an effective team leader: expertise that commands respect; teaching methods that drive pupils to want to know more; organizational skills and the ability to coordinate a network of moving parts; setting an example of patience and perseverance in the face of challenges and setbacks; encouraging team members to reflect on their own learning and their roles within the team; and finally, the acuity to select members of team that have their own expert skill sets and personality types that mesh together naturally. That was one of the most valuable and translatable lessons I learned during my two weeks with the Uganda Spine Surgery Mission.
So that's it! Time to sign off. Tomorrow the team flies back to London and then on to our respective home cities. It was a privilege to be part of the 2013 Spine Surgery Mission, and I look forward to hearing about all the successes of the 2014 trip!
Quotes of the day:
"We still have a wottle of bine"
"Six numb bums"

























 RSS Feed
RSS Feed
