The next day, we went to the hospital one last time to round on our patients before taking the bus to Entebbe, where many of us began the trip back home.


Jordan strikes again with stickers and balloons.

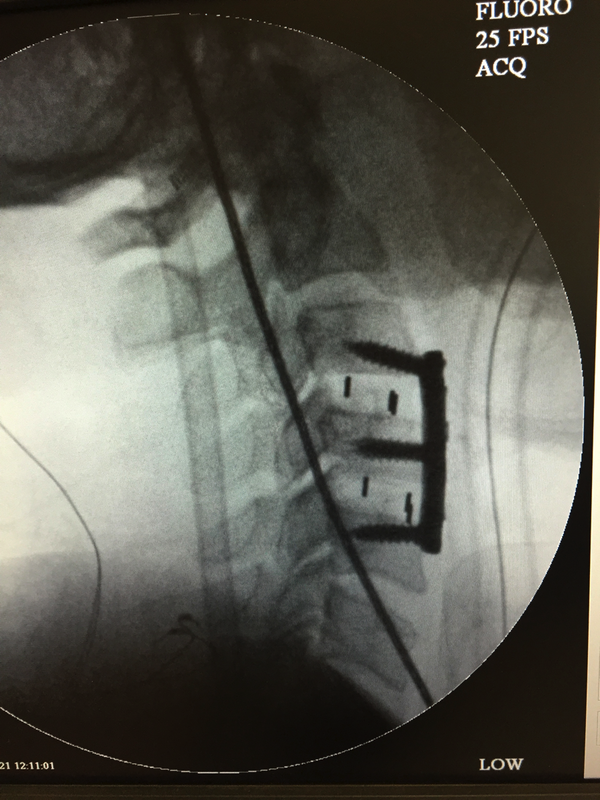
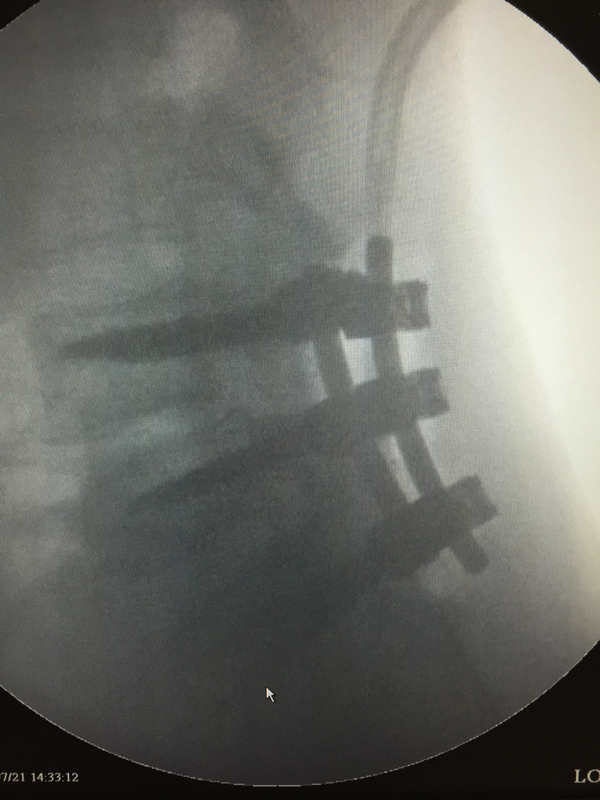
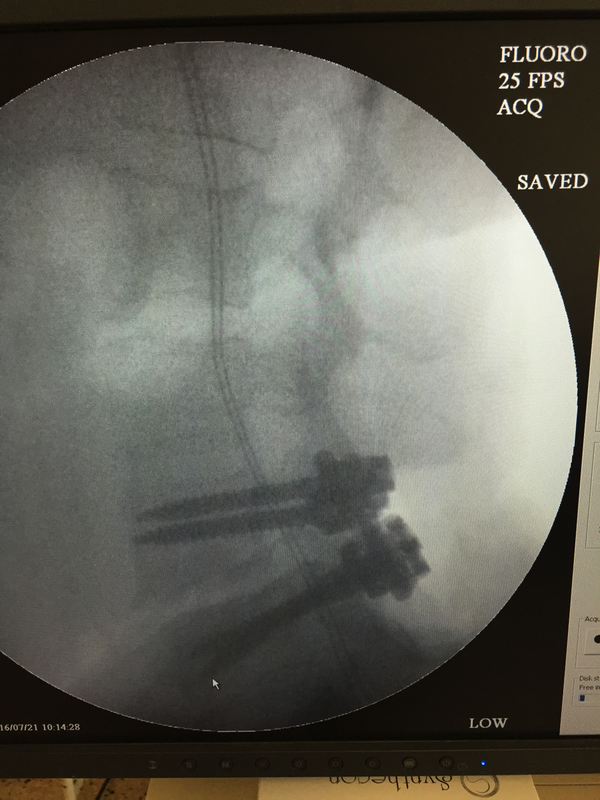
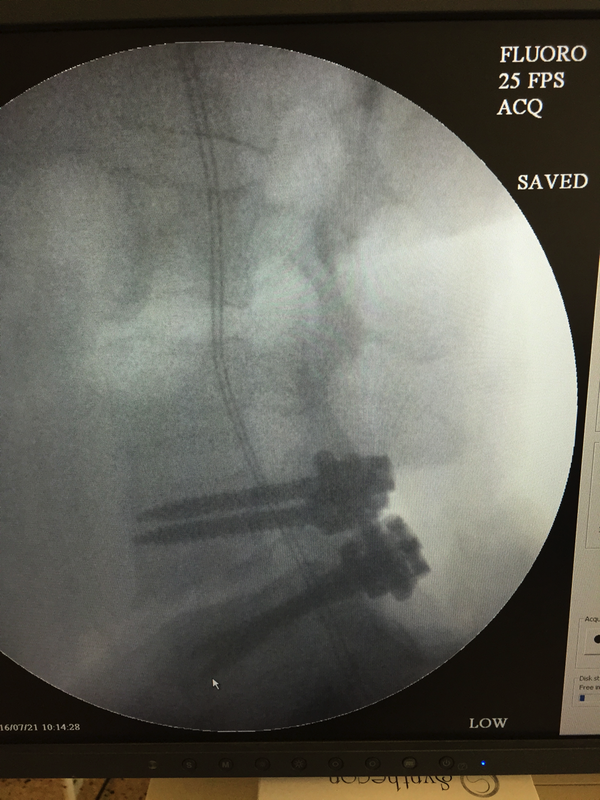
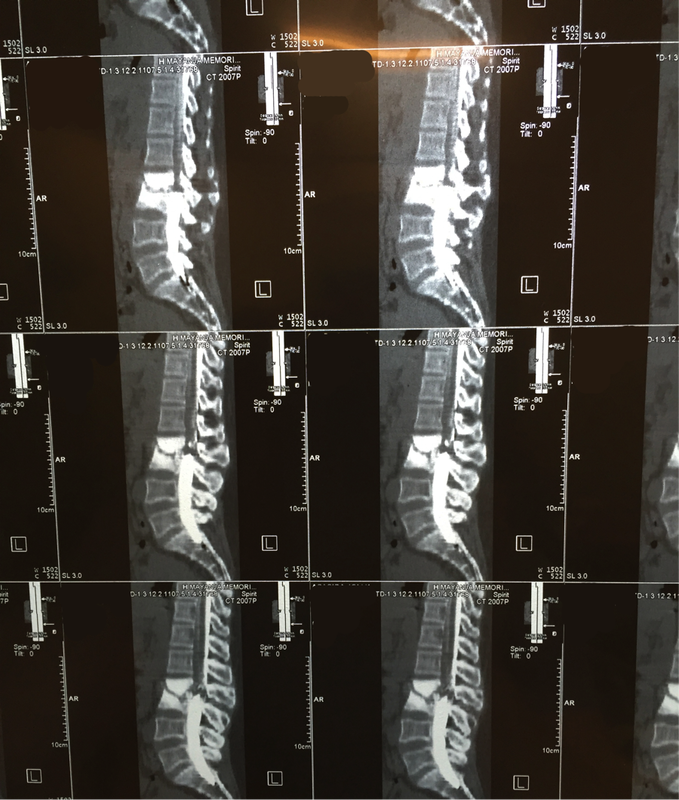
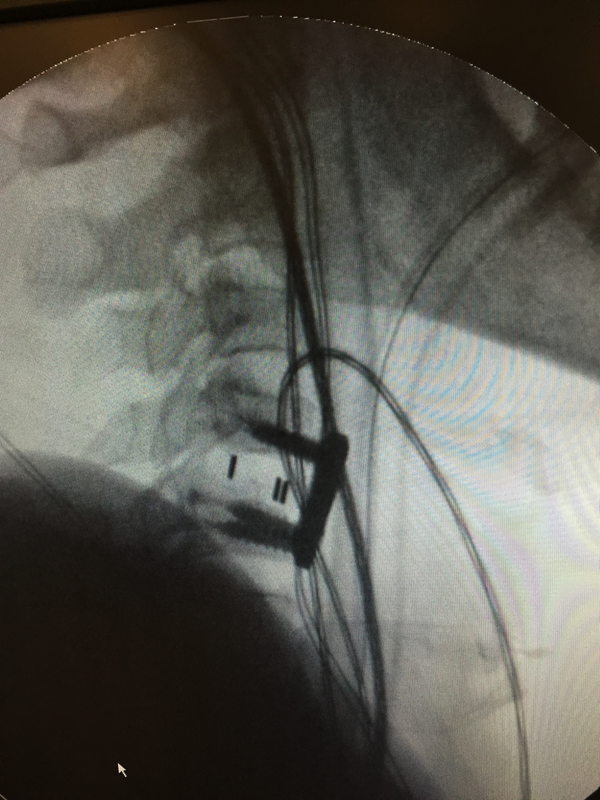
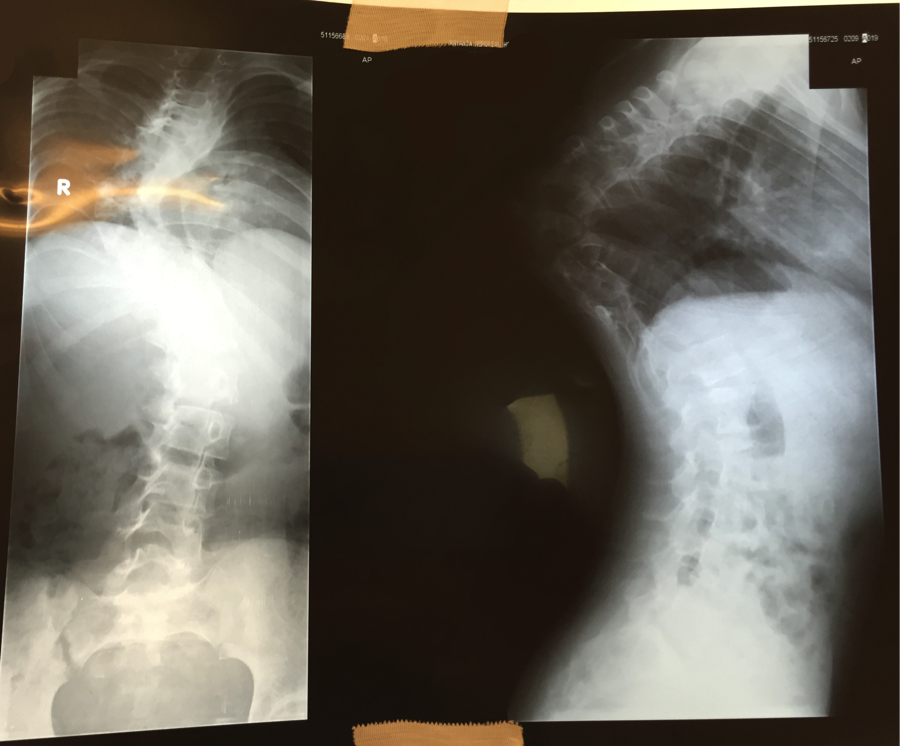
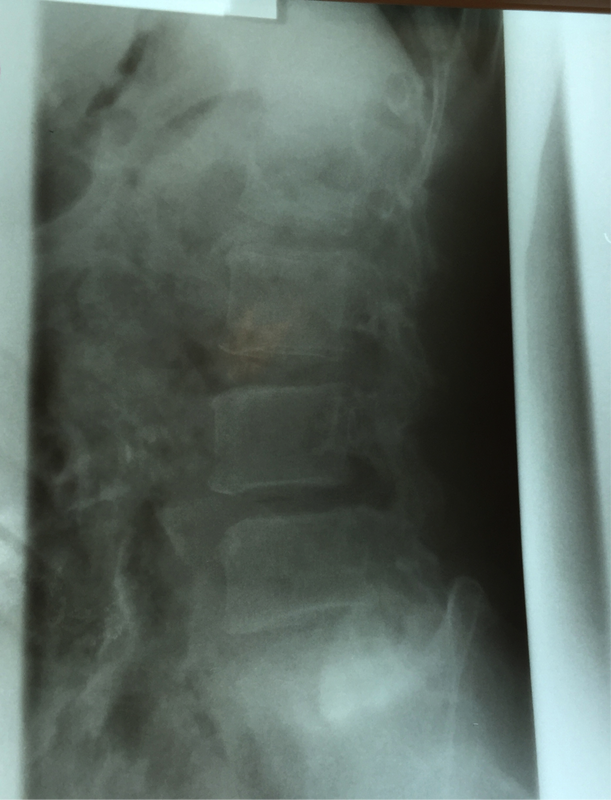
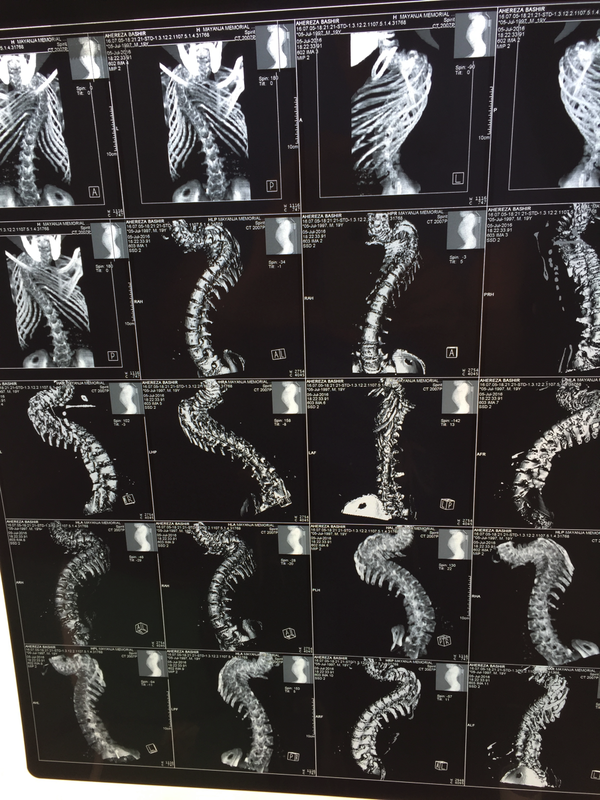
Priscilla (our scoliosis patient who had surgery Wednesday) is recovering well and standing up straight. The pain tolerance and determination of many of our patients in Uganda has been astounding. None of them have had any IV pain medications post-operatively, yet most are up and about the first day after surgery.
On the bus ride back to Entebbe, we took a scenic shortcut to avoid “jam” (which is what they call traffic in Uganda). Not only did we shave an hour or so off of the 6-hour drive, we also were treated to some nice views of the countryside.
On the bus ride back to Entebbe, we took a scenic shortcut to avoid “jam” (which is what they call traffic in Uganda). Not only did we shave an hour or so off of the 6-hour drive, we also were treated to some nice views of the countryside.

Megan: “Are there any liquor stores around here?”
We stopped by the equator line on the way to Entebbe for coffee and pictures. They have an interesting set up at the equator line with three bowls: one in the northern hemisphere, one on the equator line, and one in the southern hemisphere – all three no more than 10 feet away from one another. When water is allowed to drain from each of the bowls, the resulting water funnel twists in opposite directions on the north vs. the south side, while the water draining from the bowl directly on the equator line doesn’t seem to spin at all. A bit hard to believe at first, but we saw it with our own eyes, and even switched the bowls around to be sure it wasn’t a trick.
We stopped by the equator line on the way to Entebbe for coffee and pictures. They have an interesting set up at the equator line with three bowls: one in the northern hemisphere, one on the equator line, and one in the southern hemisphere – all three no more than 10 feet away from one another. When water is allowed to drain from each of the bowls, the resulting water funnel twists in opposite directions on the north vs. the south side, while the water draining from the bowl directly on the equator line doesn’t seem to spin at all. A bit hard to believe at first, but we saw it with our own eyes, and even switched the bowls around to be sure it wasn’t a trick.
 |  |
With that, the trip – and the blog - have come to an end. This mission has been a unique and transformative experience for me in many ways, and I have taken from Uganda many lessons and memories that will surely stay with me for the rest of my life.
As a special sign off, we leave you with a fantastic video that Michelle has put together to chronicle the July 2016 Mission.
Wishing everyone in Uganda and elsewhere a safe and happy year. Thank you to the many people who came together to make this trip possible.
https://www.youtube.com/watch?v=262wUxLGBeI&feature=youtu.be
With that, the trip – and the blog - have come to an end. This mission has been a unique and transformative experience for me in many ways, and I have taken from Uganda many lessons and memories that will surely stay with me for the rest of my life.
As a special sign off, we leave you with a fantastic video that Michelle has put together to chronicle the July 2016 Mission.
Wishing everyone in Uganda and elsewhere a safe and happy year. Thank you to the many people who came together to make this trip possible.
https://www.youtube.com/watch?v=262wUxLGBeI&feature=youtu.be









































 RSS Feed
RSS Feed
