Day 4: Murphy StrikesBreakfast was like the calm before the storm; no one truly knew what was going to happen, but we knew it would be a busy day. We had planned one instrumentation and fusion and one posterior lumbar instrumentation and fusion for the morning, and occiput (bone at the bottom of your skull) and C3 vertebra (the third vertebra in the neck) and anterior cervical discectomy and fusion (removal of the disc). Two long cases, and two short cases sounds ideal, but as Murphy’s Law states “anything that can go wrong, will go wrong, at the worst possible moment”.
We arrive at the hospital and immediately break into our separate groups; rounds and OR. Dr. Villarreal, Dr. Kisinde, Dr. Hisey, Sydnie and I all made our way down to the surgical ward, where we saw all of the previous surgical patients. All the patients were doing fantastic, and some, such as Jecinta (who had surgery on Tuesday) was up and walking with the help of our lovely physical therapist, Michelle. Others, such as Clency (one of the two little girls who had surgery on Tuesday) was doing better than she was previously, but still wasn’t doing as well as we had all hoped she would. With a little bit of encouragement and a few painkillers to make her more comfortable and alleviate her pain from such a large surgery, we hoped to see her begin to improve. With our rounds rapidly hitting its conclusion for the day, we returned to the OR where Dr. Hisey went to the one operating room to begin, while Dr. Villarreal went to join Dr. Lieberman in the other.
However, life doesn’t always intend for things to move smoothly, and always like to keep you on your toes.
Once Dr. Hisey entered his operating room with everyone who was going to assist him, they noticed the anesthesia machine was not working properly, saying there was no oxygen. Now, while a patient is sedated, the machine helps them breathe by filling their lungs with oxygen, so the machine saying there isn’t any is a rather significant problem. The technicians worked as hard as they could to get the machine up and running, and after about an hour of hard work, they finally managed to fix it! Now, as they went to retrieve the patient, they couldn’t find him. It wasn’t a matter of he wasn’t in hospital, as he was here and waiting in the back for the machine to be fixed, but more a matter of he just walked off for a bit. We frantically searched for what felt like an eternity (but was more like 5 minutes) and he just came back, all ready as long as we were, so we set to work.
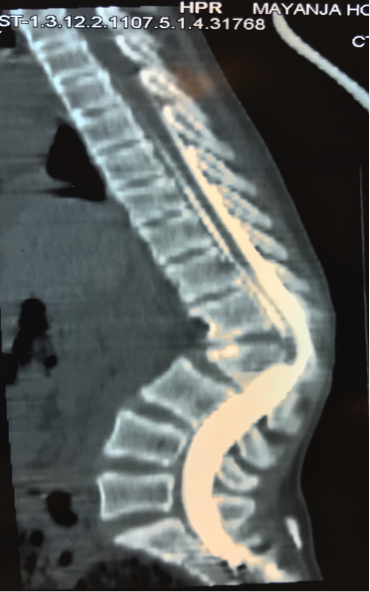
Two cases would eventually turn to three, as Dr. Hisey finished his first case, and moved onto the second, while Dr. Lieberman and Dr. Villarreal continued work on case; a young girl named Promise in need of a large instrumentation and fusion procedure, which required caution due to the shape of her scoliosis, and the size (her T5 vertebra to her L3 vertebra). With one this size and severity, caution must be taken to prevent loss of movement in her legs, or further damage to her nerves.
Cases two and three became our final case, case four. This one was on a young man named Stephano, which we knew would take a while to complete. You see, his diagnosis was an interesting one, as the bone at the base of his skull, the occiput, fused on its own to his very top vertebra, C1 (Fun fact, it’s also known as “Atlas” because it holds supports the globe of your head, after the Greek myth Atlas, who holds the world up on his shoulders). This auto-fusion, in turn, caused compression on his spinal cord and further complications, such as sudden weakness in his right side. This procedure would (as expected), turn out to be a long case, as it must be approach with extreme caution. It was planned to fuse his occiput bone to his C3 vertebra, and to decompress the spinal cord, in an attempt to have him regain motor function
The night came to a late close, and we prepared to return back to the hotel for a well-earned night of sleep and rest, realizing that week 1 was slowly approaching an end. Little did we know, however, that while today was stressful, the rest of the week would hold more interesting surprises for us, never letting us relax for too long.
We arrive at the hospital and immediately break into our separate groups; rounds and OR. Dr. Villarreal, Dr. Kisinde, Dr. Hisey, Sydnie and I all made our way down to the surgical ward, where we saw all of the previous surgical patients. All the patients were doing fantastic, and some, such as Jecinta (who had surgery on Tuesday) was up and walking with the help of our lovely physical therapist, Michelle. Others, such as Clency (one of the two little girls who had surgery on Tuesday) was doing better than she was previously, but still wasn’t doing as well as we had all hoped she would. With a little bit of encouragement and a few painkillers to make her more comfortable and alleviate her pain from such a large surgery, we hoped to see her begin to improve. With our rounds rapidly hitting its conclusion for the day, we returned to the OR where Dr. Hisey went to the one operating room to begin, while Dr. Villarreal went to join Dr. Lieberman in the other.
However, life doesn’t always intend for things to move smoothly, and always like to keep you on your toes.
Once Dr. Hisey entered his operating room with everyone who was going to assist him, they noticed the anesthesia machine was not working properly, saying there was no oxygen. Now, while a patient is sedated, the machine helps them breathe by filling their lungs with oxygen, so the machine saying there isn’t any is a rather significant problem. The technicians worked as hard as they could to get the machine up and running, and after about an hour of hard work, they finally managed to fix it! Now, as they went to retrieve the patient, they couldn’t find him. It wasn’t a matter of he wasn’t in hospital, as he was here and waiting in the back for the machine to be fixed, but more a matter of he just walked off for a bit. We frantically searched for what felt like an eternity (but was more like 5 minutes) and he just came back, all ready as long as we were, so we set to work.
Two cases would eventually turn to three, as Dr. Hisey finished his first case, and moved onto the second, while Dr. Lieberman and Dr. Villarreal continued work on case; a young girl named Promise in need of a large instrumentation and fusion procedure, which required caution due to the shape of her scoliosis, and the size (her T5 vertebra to her L3 vertebra). With one this size and severity, caution must be taken to prevent loss of movement in her legs, or further damage to her nerves.
Cases two and three became our final case, case four. This one was on a young man named Stephano, which we knew would take a while to complete. You see, his diagnosis was an interesting one, as the bone at the base of his skull, the occiput, fused on its own to his very top vertebra, C1 (Fun fact, it’s also known as “Atlas” because it holds supports the globe of your head, after the Greek myth Atlas, who holds the world up on his shoulders). This auto-fusion, in turn, caused compression on his spinal cord and further complications, such as sudden weakness in his right side. This procedure would (as expected), turn out to be a long case, as it must be approach with extreme caution. It was planned to fuse his occiput bone to his C3 vertebra, and to decompress the spinal cord, in an attempt to have him regain motor function
The night came to a late close, and we prepared to return back to the hotel for a well-earned night of sleep and rest, realizing that week 1 was slowly approaching an end. Little did we know, however, that while today was stressful, the rest of the week would hold more interesting surprises for us, never letting us relax for too long.

































 RSS Feed
RSS Feed
